Date: 09-14-2025 at 06:31 PM
The Challenge of Measuring LTV in Healthtech
Customer LTV is easier to measure in ecommerce and business where the customer is the end user. But it creates confusion when your customer is not an end user. Or a user can become your customer between a day to year? It is difficult to measure the metric.
Example: We first met Md. Tanvir, a 35-year-old, during one of our health camps. His fasting blood glucose came out at 223 mg/dl, which immediately raised concerns. Our AI engine also flagged him as high risk for diabetes—not just because of this reading, but also considering other health parameters and the fact that both his parents were diabetic. Naturally, he was worried. We reassured him, explained that a single spike doesn’t confirm diabetes, and advised an HbA1c test for better clarity. At the same time, we encouraged him to cut down on sugar and increase physical activity.
A week later, he returned for another screening. This time, his fasting glucose had dropped to 183 mg/dl. The relief on his face was unmistakable—his small lifestyle changes were already making a difference.
A few days later, Tanvir reached out again—this time for his brother. He wanted lab diagnostics, including a full-body checkup. He shared his brother’s prescription from a local doctor, and based on the symptoms, we recommended additional tests like Vitamin B12 and Vitamin D. As usual, while collecting samples, our team also recorded the primary vitals—a free service we provide for every customer.
That’s when things took a serious turn. Our system detected alarming red flags:
- Resting heart rate: 130 bpm
- Respiratory rate: 33 breaths/min
- Blood pressure: unusually low
For a young man of 35, these numbers were dangerous. We immediately advised him to consult a good physician without delay.
It turned out that an overdose of medication for a simple viral fever had pushed him into this condition. Fortunately, following our suggestion, he consulted a doctor from Medanta, who prescribed further lab tests. And here’s something that struck us—despite the urgency, Tanvir actually waited an extra day just so he could get those tests done with Jilo Health.
Since that first health camp, he has already done ₹3,000+ worth of labs with us. For context, we spent ₹53 to acquire him (a relatively high acquisition cost at this stage). And remember, we don’t even offer doctor consultations or medicines—just diagnostics through partner labs.
So here’s the question we keep coming back to: How do you measure a customer’s lifetime value (LTV) in healthtech?

Health Camp in Gandhi Maidan
Because unlike e-commerce, where customer behavior is predictable and transactional, in healthcare a person may need you once, occasionally, or for life. One day it’s just a sugar test. Another day, it’s a life-threatening red flag that turns into years of ongoing engagement.
Why Teleconsultation is a Flawed Business Model in Healthtech
Teleconsultation was once considered a promising solution in the healthtech ecosystem, but it has fundamentally failed to scale in a sustainable way—especially in a country like India. The reason lies in the very nature of healthcare itself.
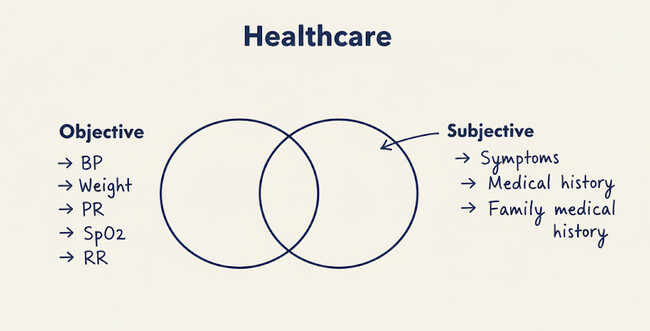
Healthcare is built upon two types of data: objective and subjective. Objective data includes health vitals, biomarkers, and laboratory parameters, while subjective data covers symptoms, medical history, and family conditions. Teleconsultation, by its very design, captures only the subjective dimension. Without objective data, any healthcare solution is inherently incomplete.
This limitation is starkly evident in a country like India, where the shortage of healthcare professionals is immense. A purely digital model, focused on teleconsultation, cannot bridge the gap because it excludes critical diagnostic inputs that are necessary for safe and accurate care.
The Flaws of Teleconsultation in Practice
Consider a simple scenario: a patient with fever books a teleconsultation through Practo. During the video or audio call, the patient shares symptoms and history. The doctor, relying solely on this subjective data, writes a prescription. However, essential vitals—weight, blood pressure, SpO₂, respiratory rate, pulse rate—are missing.
This practice is inherently flawed. Drug compositions and dosages depend on objective parameters like age and weight. Metabolism, too, influences how medicines are absorbed and processed. Prescribing without objective data risks inaccuracy and even harm.
Thus, telemedicine may have niche applications, but as a standalone solution in primary care, it remains incomplete. Its failure in India is also cultural: in Bharat (non-metro India), patients fundamentally trust physical or “phygital” (physical + digital) care over digital-only approaches.
Economics of Primary Healthcare
Another reason teleconsultation cannot be a large business in India is its limited role in the overall healthcare value chain. In the primary care continuum, consultation is a small expenditure, while diagnostics and medication constitute the largest cost components.
For example, a patient with hypertension in Patna undergoes lab tests confirming the diagnosis. The doctor prescribes branded medication. If incentivized by pharma companies, doctors may prescribe high-cost brands such as Telmikind-AM, which costs ₹160 for 20 tablets. In contrast, the generic equivalent costs barely ₹20.5. Since chronic conditions like hypertension require lifelong medication, affordability becomes critical.
Read the full essay: https://www.sumanjha.com/post/how-do-you-measure-life-time-value-of-a-customer-in-healthtech-healthcare